
ADHA supports dental hygienists practicing autonomously to the full extent of their education and licensure. The association advocates for expanded direct access, allowing hygienists to assess, prevent, and treat patients without prior dentist authorization to improve access to preventive oral care. This autonomy recognizes dental hygiene diagnosis as essential and supports modern workforce models while maintaining high standards of education and patient safety.
Direct Access
ADHA defines direct access as a dental hygienist’s ability to assess patients, initiate treatment, provide care without a dentist present, and maintain an ongoing provider–patient relationship. Direct access empowers hygienists to expand access to preventive care, particularly for underserved populations, and helps reduce oral health disparities. ADHA also provides a state-by-state Direct Access resource outlining applicable laws.
Learn More About Direct ACCESS
Scope of Practice
ADHA supports dental hygienists practicing to the full extent of their scope to improve access to care. Because permitted functions and supervision vary by state, ADHA provides state-specific resources to help hygienists understand legal requirements, advocate for expanded authority, and deliver safe, effective care aligned with their education and licensure.
The Oral Health Workforce Research Center also offers an interesting overview of the variation in dental hygiene scope of practice by state.
Medicaid Reimbursement
As of 2025, 19 states have statutory or regulatory language allowing their Medicaid programs to reimburse dental hygienists for services rendered. ADHA advocates at both the state and federal levels to ensure private and government insurance programs properly reimburse dental hygienists.
ADHA offers a resource detailing the language that permits state Medicaid programs to reimburse dental hygienists.
View Medicaid Reimbursement States
Restorative Services
Dental hygienists may perform certain restorative services, with specific duties and supervision requirements determined by state law. These services are typically supportive, involving placement and finishing of restorative materials after a dentist prepares the tooth. Hygienists often obtain a restorative certificate through state-approved continuing education. ADHA provides a state-by-state chart outlining permitted restorative duties.
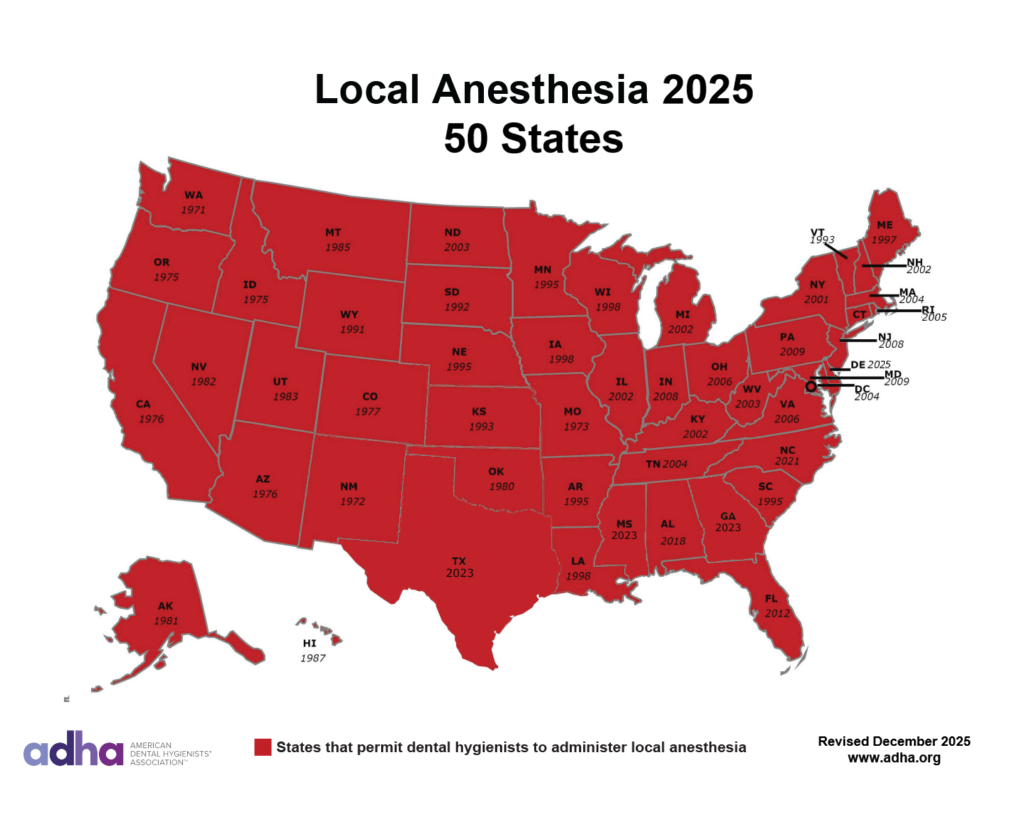
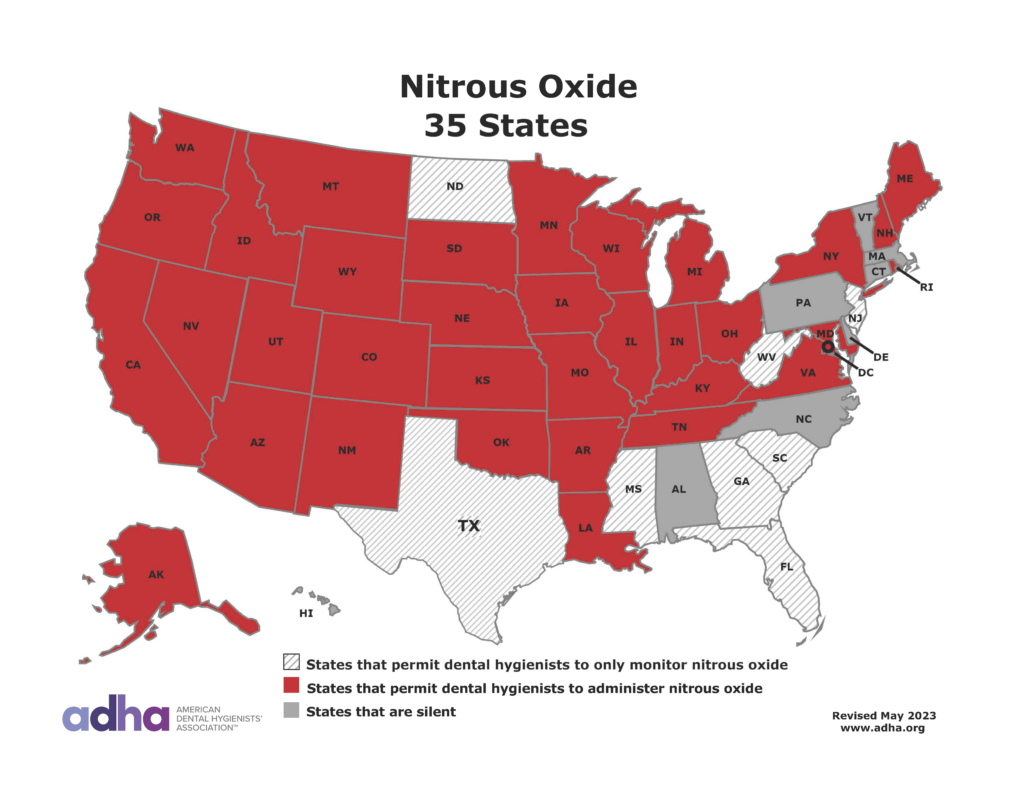
Anesthesia
As of August 2025, all states permit dental hygienists to administer local anesthesia, marking a major milestone for the profession after decades of ADHA advocacy. This ensures patients can receive comfortable, pain-free care. Additionally, 35 states allow hygienists to administer nitrous oxide, and eight permit monitoring. ADHA provides a state chart outlining anesthesia regulations.
Dental Hygiene Diagnosis
Dental hygiene diagnosis involves identifying patients’ oral health needs based on evidence-based assessment and forms the foundation of the dental hygiene care plan. ADHA recognizes dental hygiene diagnosis as an essential component of education and scope of practice and supports curricula that ensure competency in the full process of care.
Learn more about Dental Hygiene Diagnosis in ADHA’s White Paper Dental Hygiene Diagnosis: Defining the Essential Role of Diagnostic Decision Making in Dental Hygiene.
Silver Diamine Fluoride
Silver diamine fluoride (SDF) 38% has been used extensively outside the United States for many years for caries control. SDF is a colorless liquid, or tinted blue, containing silver particles and fluoride ion that at pH 10 or 13 is 25% silver, 8% ammonia, 5% fluoride (44,800 ppm), and 62% water. This is referred to as 38% SDF.
ADHA provides a state-by-state chart for Silver Diamine Fluoride (SDF) use.